Articles
P E E R – R E V I E W E D · D O S E – R E S P O N S E : A N I N T E R N A T I O N A L J O U R N A L · V O L .2 3 ( 3 ) · 2 0 2 5
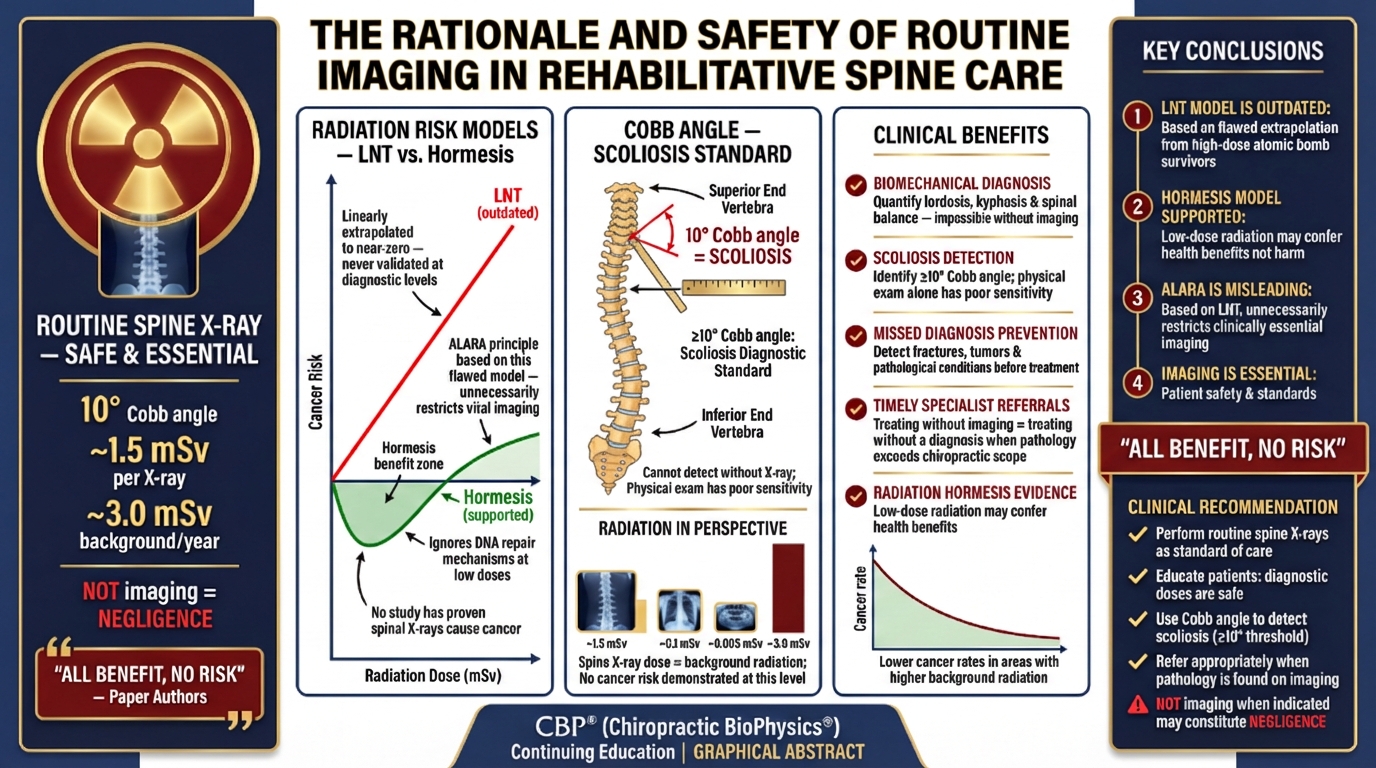
Are Spine X-Rays Really Dangerous? New Research Says the Fear is Unfounded — and Withholding Them May Be Negligent
A Landmark Commentary on the Safety and Necessity of Routine Spinal Radiography in Rehabilitative Care
By Paul A. Oakley, Jason W. Haas & Deed E. Harrison | Dose-Response 2025 | DOI: 10.1177/15593258251374411
97%OF ‘HEALTHY’ RECRUITS HAD PATHOLOGIC X-RAY FINDINGS |
1 in 32CHIROPRACTIC PATIENTS HAVE MALIGNANCY ON X-RAY |
0EVIDENCE FOR CANCER RISK AT DIAGNOSTIC X-RAY DOSES |
73%OF PATIENTS EXPECT X-RAYS FOR DIAGNOSIS |
|---|
The Invisible Epidemic: Undiagnosed Spinal Deformity
For decades, clinical guidelines have warned practitioners away from routine spinal X- rays, citing radiation risk and limited diagnostic utility. A new commentary published in Dose-Response: An International Journal by Oakley, Haas, and Harrison (2025) makes the case that these guidelines are not just wrong — they may be contributing to a silent epidemic of missed spinal diagnoses and, in some circumstances, rising clinician liability.
The paper opens with a striking observation: postural alignment is a critical determinant of health status. Its degradation is directly linked to deformity-caused back pain, neurologic compromise, osteoarthritic degeneration, and reduced quality of life. Yet the diagnostic tool best suited to detect and quantify spinal deformity — the plain radiograph
— is precisely what current guidelines discourage.
“The prime obstacle to routine X-ray imaging lies with the presumed threat of cancer, however, this is dogma.”
— Oakley, Haas & Harrison, 2025
Part I: Debunking the Radiation Cancer Myth
The Linear No-Threshold (LNT) Model — Science or Misconduct?
The fear of X-ray radiation in clinical practice traces back to the Linear No-Threshold (LNT) hypothesis — the assumption that any dose of ionizing radiation, no matter how small, carries a proportional cancer risk. The authors trace this model’s origin to the work of Hermann Muller, whose Nobel Prize-winning research on radiation-induced genetic mutations was later found to involve scientific misconduct. Muller suppressed data showing that low doses were harmless or even beneficial.
Despite having no empirical foundation at diagnostic dose levels — typically well below 200 mrem — the LNT model became incorporated into radiation safety policy, ultimately producing what the authors call radiophobia: an irrational fear of diagnostic X-rays.
2.5 yrs
Longer life expectancy in high background radiation areas (>180 vs <100 mrem/yr)2.5 yrs
Longer life expectancy in high background radiation areas (>180 vs <100 mrem/yr)
200M×
More DNA damage from human metabolism (ROS/H₂O₂) than from background radiation200M×
More DNA damage from human metabolism (ROS/H₂O₂) than from background radiation
<200 mrem
Dose threshold — below which NO evidence supports radiation-induced cancer<200 mrem
Dose threshold — below which NO evidence supports radiation-induced cancer
Radiation Hormesis: Low Doses May Be Beneficial
The authors cite substantial evidence for radiation hormesis — the J-shaped dose- response relationship in which low doses of radiation stimulate biological repair mechanisms and may confer health benefits. Populations living in areas of higher natural background radiation (above 180 mrem/year) demonstrate a life expectancy that is 2.5 years longer than those in low-background areas (below 100 mrem/year).
Meanwhile, normal human metabolism generates reactive oxygen species (ROS) that inflict approximately 200 million times more genetic damage per cell per day than background radiation. The body’s DNA repair systems efficiently manage both. A diagnostic spinal X-ray delivers a dose roughly comparable to a cross-country flight — an exposure no one requires informed consent for.
Part II: The Clinical Case for Routine Imaging
What Radiography Reveals — and Physical Exam Cannot
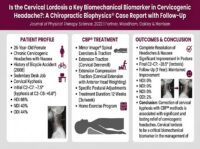
Biomechanical diagnosis of the spine — the cornerstone of evidence-based corrective chiropractic care — requires quantitative measurement of spinal alignment parameters. Table 1 in the paper provides clinically validated thresholds for 12 spinal parameters, each linked to specific pain states, disability levels, or structural diagnoses:
| Region | Parameter | Normal/Ideal | Clinical Threshold | Consequence |
|---|---|---|---|---|
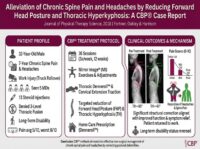
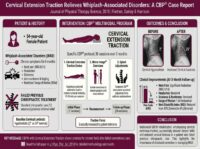
| Cervical | Anterior Head Translation | <15 mm | >25 mm = pain/ disability;
>40 mm = severe disability |
Neck pain, radiculopathy |
| Cervical | Lordosis
Cobb C2-C7 |
30–39° | <20° = 9-10× headache/pain risk;
<0° = neurovascular deficit |
Headaches, chronic pain |
| Cervical | ARA C2-C7 | >34° pain-free | <29° acute pain;
<22° chronic pain threshold |
Acute/chronic neck pain |
| Thoracic | Kyphosis
Cobb T4-T12 |
20–40° | >45° pain/self-image issues;
>60° = deformity/disability |
Deformity, disability |
| Thoracic | Cobb T5-T12 | 33° limit | >33° = hyperkyphosis | Thoracic Pain |
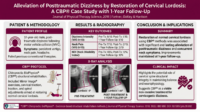
| Lumbar | Lordosis
Cobb T12-S1 |
65° average | <57° = chronic pain threshold | Chronic low back pain |
| Pelvis | Pelvic Tilt | <20° | >20° deformity;
>25° disability |
Pelvic deformity, pain |
| Full Spine (Lat) | Sagittal Vertical Axis | >40 mm deformity;
>50 mm disability; >95 mm severe |
Falls, disability, QOL reduction | |
| Full Spine (AP) | Scoliosis Cobb | <10° | >10° mild;
>20° moderate; >40° severe; >50° surgical |
Pain, deformity, surgery |
| Full Spine (AP) | Coronal Plumbline | Midline | >40 mm = coronal imbalance | Compensatory deformity |
In an analysis of 100 consecutive chiropractic patients, the authors report: only 12% had ideal cervical lordosis, 64% had curves straighter than 22°, 44% had anterior head translation exceeding 25 mm, 20% had sagittal vertical axis imbalance above 50 mm (meeting the threshold for Adult Spinal Deformity), and 15% had complete cervical kyphosis — associated with an 18-fold increased risk of neck pain.
Five Real Patients: Diagnoses Only Possible With X-Ray
The paper presents five clinical case studies demonstrating radiographic findings that fundamentally altered patient management. Each X-ray set includes biomechanical analysis lines using the Harrison Posterior Tangent Method.
Case 1 — 37yo Male: Posture & Hip Tightness
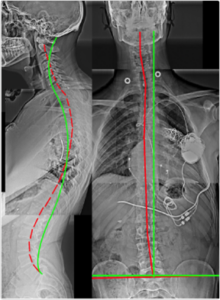
Figure 1. Right Thoracic Lean, Right Head Translation, Increased Pelvic Tilt, Lumbar Hyperlordosis, Thoracic Hyperkyphosis, Anterior Head Translation, Cervical Hypolordosis. Multiple intersecting deformities — none detectable without X-ray
Case 2 — 32yo Female: Chronic Back Pain (6/10)
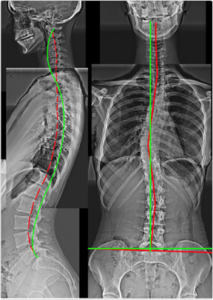
Figure 2. Scoliosis, Cervical Kyphosis, Thoracic Hypokyphosis, Increased Pelvic Tilt, Lumbar Hyperlordosis. Scoliosis is invisible on physical examination — only visible on AP weight-bearing X-ray.
Case 3 — 46yo Male: Chronic Neck & Back Problems
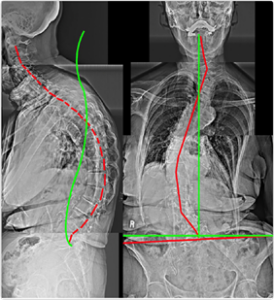
Figure 3. Thoracic Hyperkyphosis, Posterior Thoracic Translation, Anterior Head Translation, Cervical Hypolordosis, Anatomical Leg Length Discrepancy. Leg length discrepancy causes compensatory scoliosis — only confirmed on AP X-ray.
Case 4 — 83yo Female: Unable to Straighten Up
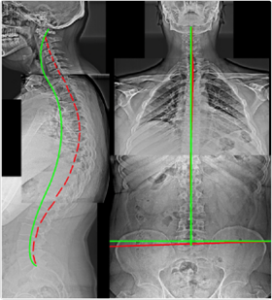
Figure 4. Severe Scoliosis, Severe Thoracolumbar Kyphosis, Anterior Head Translation, Right Lateral-Listhesis L4 on L5. The lateral listhesis — a serious structural finding — was entirely unknown prior to imaging.
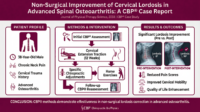
Case 5 — 64yo Female: Chronic Pain 8/10
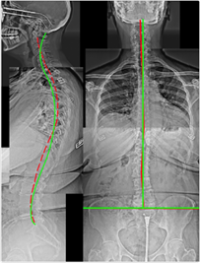
Figure 5. Lumbar Scoliosis, Right Head Translation, Upper Thoracic Hyperkyphosis, Lower Thoracic Lordosis (reversed curvature), Anterior Head Translation, Cervical Hypolordosis. Pain of 8/10 fully explained by radiographic findings.
The Medico-Legal Argument: When Not Imaging is Negligent
Perhaps the most clinically significant section of the paper addresses the standard-of-care implications. The authors draw on data from Beck et al., which screened 1,172 consecutive chiropractic patients and found:
3.1%
Malignancy (1 in 32 patients)3.1%
Malignancy
(1 in 32 patients)
6.6%
Fracture (1 in 15 patients)6.6%
Fracture
(1 in 15 patients)
0.8%
Abdominal Aortic Aneurysm (1 in 125)0.8%
Abdominal Aortic Aneurysm (1 in 125)
0.6%
Atlantoaxial Instability (1 in 167 patients)0.6%
Atlantoaxial Instability
(1 in 167 patients)
⚠ The Authors State: “The failure to radiographically diagnose spinal deformity is argued to be negligence in many cases.” When the risk from a diagnostic X-ray is zero — and the risk of missed malignancy, fracture, or instability without imaging is 1–7% — withholding the diagnostic tool that could detect them does not serve patient welfare.
Additionally, 73% of patients actively expect imaging as part of their diagnostic workup. Denying this expectation — without scientific justification — erodes patient confidence and clinical credibility.
A Call to Update Clinical Guidelines
The paper concludes with a direct call to action: current spine care guidelines must be revised to include a specific exception for patients undergoing corrective rehabilitative interventions. For these patients — the very population seen in CBP® and evidence- based corrective chiropractic clinics — radiographic evaluation is not optional. It is the scientific and ethical standard of care.
□ Bottom Line: Routine spinal X-rays are safe, scientifically validated, biomechanically essential, and clinically mandatory for corrective spine care. The cancer risk narrative is unfounded. The diagnostic benefit narrative is overwhelming. This paper provides the scientific and legal justification for maintaining imaging as a core clinical tool.
“Current guidelines must include a caveat for contemporary biomechanical evaluation and its consequent specific treatments and should recommend routine radiographic imaging for spine patients undergoing corrective rehabilitative interventions.”
— Oakley PA, Haas JW, Harrison DE. Dose-Response. 2025;23(3):1-18.
Suffering from neck pain, back pain or poor posture?
Share This Story:
📚 Cite This Publication
Oakley PA, Haas JW, Harrison DE. The Rationale and Safety of Routine Imaging in Rehabilitative Spine Care: Delayed Radiographs for Patients Presenting With Spine Disorders is Debatable. Dose-Response: An International
Journal. 2025;23(3):1-18. DOI: 10.1177/15593258251374411
Access: journals.sagepub.com/home/dos | idealspine.com | cbpnonprofit.com
#CBP #SpineHealth #SpinalImaging #ChiropracticBioPhysics #RadiationSafety #SpinalDeformity #Kyphosis #Scoliosis #PosturalHealth #EvidenceBasedCare
About the Authors & CBP Non-Profit
This study was conducted by researchers including Dr. Deed E. Harrison, President of CBP NonProfit Inc. CBP® (Chiropractic BioPhysics®) is one of the most researched chiropractic techniques in the world, focusing on optimal posture and spinal alignment as the primary goals of care. By combining physics, geometry, and biology, CBP® doctors aim to restore normal spinal mechanics to improve overall health.
Recent Posts
CONTACT CBP
CBP Seminars, Inc.
21863 Thorsten Avenue Suite 207
Caldwell, ID 83605
Phone: 208-939-0301
Fax: 208-209-6009
Email: [email protected]
Web: idealspine.com
LATEST ARTICLES
CONTACT CBP
CBP Seminars, Inc.
1160 Taylor Street Suite 100
Meridian, ID 83642
Phone: 208-939-0301
Fax: 208-209-6009
Email: [email protected]
Web: idealspine.com