Technique
What is CBP®?
In December 1980, Chiropractic BioPhysics® or CBP® Technique, was originally named by Drs. Donald Harrison, Deanne Harrison, and Daniel Murphy for “physics applied to biology in chiropractic”.
 Since that time, Drs. Donald and Deed Harrison, (along with a number of other contributors) have authored Seven CBP® Texts Books and published more than 341 scientific studies investigating different aspects of CBP®.1-7
Since that time, Drs. Donald and Deed Harrison, (along with a number of other contributors) have authored Seven CBP® Texts Books and published more than 341 scientific studies investigating different aspects of CBP®.1-7
Thus, today, CBP® Technique is one of the foremost investigated techniques in Chiropractic and both Dr. Donald and Dr. Deed Harrison are among the leaders in the profession’s researchers.
CBP® Goals of Care
CBP® Technique emphasizes optimal posture and spinal alignment as the primary goals of chiropractic care while simultaneously documenting improvements in pain and functional based outcomes (See Figure 1). The uniqueness of CBP® treatment is in structural rehabilitation of the spine and posture. In general the goals of CBP® Care are:
- Normal Front & Side View Posture
- Center of mass of head, rib cage & pelvis vertically aligned in Front and Side views.
- Normal Spinal Alignment
- Front view: vertical alignment
- Side View: Harrison Ideal or Average Spinal Model
- Normal function
- Improved Range of Motion and quality of movement,
- Improved muscle strength,
- Improved Health & Symptom Improvements
- Neck disability index
- Oswestry low back index,
- SF 36 or Health Status Questionnaire
Ideal Postural Alignment
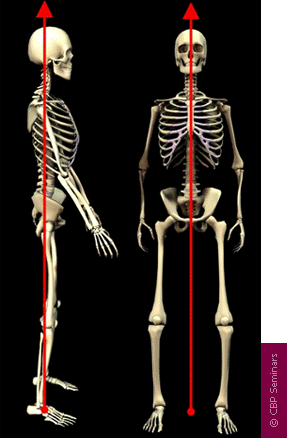
Figure 1. Ideal postural alignment is depicted in both the frontal and side views. In each view, the center of mass of the skull, thorax, and pelvis are in a vertical line with respect to gravity. In the frontal view, the spinal column is vertically aligned-a straight column- with respect to gravity. In the side view, the spine has three primary curvatures which will be described below:
1. Neck Curve – Cervical Lordosis,
2. Ribcage Curve – Thoracic Kyphosis,
3. Low back Curve – Lumbar Lordosis
Ideal Spinal Alignment: Harrison Full Spine Model
As in all fields of study dealing with the human body, i.e. physiology, hematology, anatomy, etc., there exist normal values for alignment of the spine. The Harrison Spinal Model is an evidenced based model for side view spinal alignment. It is the geometric path of the posterior longitudinal ligament or the backs of the vertebra from the 1st neck vertebra to the bottom of the lower back or top of the sacrum. See Figures 2-6 below detailing the Harrison Spinal Model.
CBP® researchers have extensively published ideal and average models for the human spinal curvatures as viewed from the side. This research has lead to the finding of the ‘Harrison Spinal Model’. This model details both Ideal and Average geometric shapes for the curves of the spine from the side. Additionally, ideal and average ranges for the spinal segmental angles for each of the spinal regions have been identified. The neck or cervical spine should have a geometric shape that approximates a ‘piece of a circle’. The ribcage or thoracic spine should have a geometric shape that approximates an oval-elliptical shape. And the low back or lumbar spine should have a geometric shape that approximates an oval-elliptical shape.26-31
These are “evidence based” models. In fact, the CBP® neck-cervical circular model27 and the low back- lumbar elliptical model29 have both been found to have discriminative validity between pain and non pain subjects. In other words, the Harrison Spinal Model has been found to be able identify pain subjects versus non-pain subjects by what their spinal x-ray shapes are.
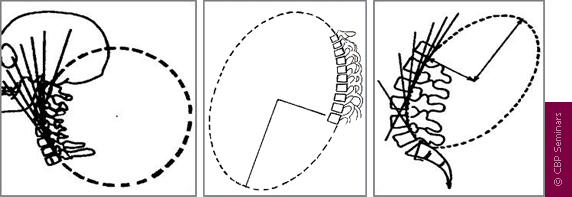
Figure 3. These three figures demonstrate the concept that each spinal region has a normal geometry or shape of the spinal curves. On the readers left is the Neck or Cervical spine-Here the shape in the neck curve should approximate a piece of a circle. In the Center is the Ribcage or Thoracic spineHere the shape in the ribcage should approximate a piece of an oval or ellipse. On the Right is the Low back or Lumbar spine. Here the shape in the low back should approximate a piece of an oval or ellipse.
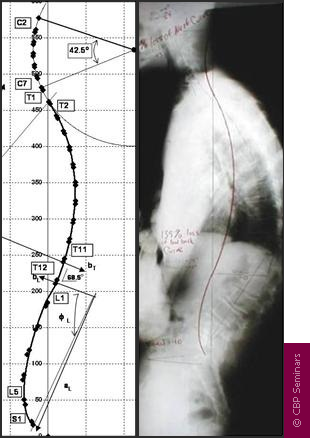
Figure 4. The Harrison Full Spine Model. On the readers left is the exact geometric model of the side view of the spinal curves as identified by Harrison and colleagues. This model can be used to determine what is wrong-abnormal with a given patients side view of the spine. For example, a full spine x-ray on the right is shown. The red-curved line represents the Harrison spinal model and this shows where the patients spinal vertebra should be lined up. It is apparent that this patient has altered spinal alignment as they do not fit even close to the Harrison Idealized Spinal Model.
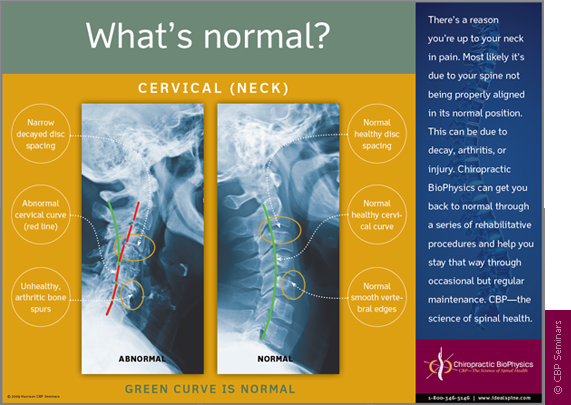
Figure 5. The Harrison Spinal Model in the Neck-Cervical region. The Harrison spinal model is depicted as the GREEN curved line in this figure. On the Right is a normal curved patient x-ray. On the Left is an abnormal curved patient x-ray; where the patients abnormal shape is shown by the Red dashed line. The Harrison Spinal Model in the neck has been shown to reasonably predict which person will have neck pain compared to normal subjects.
Figure 6. The Harrison Spinal Model in the Low back or Lumbar region. The Harrison spinal model is depicted as the RED curved line in this figure. On the Right is a normal curved patient x-ray. On the Left is an abnormal curved patient x-ray; where the patients abnormal shape is shown by the faint dashed line. The Harrison Spinal Model in the low back has been shown to reasonably predict which person will have low back pain compared to normal subjects.
X-Ray Analysis and Utilization
To establish optimal and average sagittal models, x-ray analysis and line drawing procedures are utilized. CBP® protocols require that the doctor must measure the displacements on spinal radiographs (segmental Subluxation). Both lateral-side view and anterior to posterior (AP) or frontal view CBP® x-ray line drawing procedures have been studied and found to be reliable.32-36 Furthermore, CBP® utilizes standardized x-ray positioning procedures that have been studied and found to be reliable.36
As with measures of pain intensity, range of motion, and quality of life, periodic assessment of spinal structural alignment is important to evaluate progress and determine when maximum patient improvement has been reached. In CBP® Technique, the use of initial and follow-up spinal x-rays or radiographs is deemed necessary; however, some in chiropractic have condemned the use of follow-radiographs to collect alignment data.37-39 Importantly, there is data to show that the use of medical/chiropractic x-rays constitutes a very minor health risk and in fact has been shown to be of benefit (decreased sickness and cancer mortality rates) in some studies.40-42
In reality, the only way to see what an individual patients spine alignment looks likes, is to obtain spinal imaging such as Radiography or X-ray. No-one would not take their car to the mechanic and say: Something’s wrong with my engine but don’t look under the hood–Would you? Then why would anyone want a Chiropractor to adjust-treat their spine without having an x-ray to see what the person’s spine looked like? Would You?
CBP® Postural Analysis
Previously, engineering concepts were used to describe all spinal-vertebral segmental movements as rotations and translations in 3-dimensions.10 However, Dr. Don Harrison was the first to describe abnormal postures of the head, rib cage, and pelvis in this manner.1-3,9 Figures 7 and 8 depict the twelve simple motions in six-degrees of freedom as rotations and translations of the human head, ribcage, and pelvis:
- Rotation is a turning, twisting, or tilting movement and is an angular movement
- Translation is a straight line movement (up, down, left, right, forward, backward)
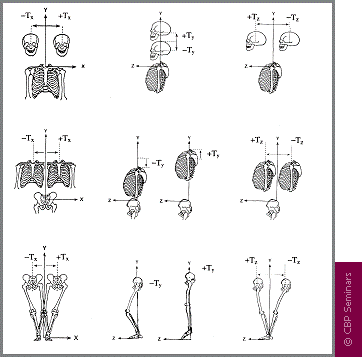
Figure 7. The possible translation postures (Tx, Ty, Tz) of the head, rib cage, and pelvis are depicted in 3-dimensions. In 1980, Dr. Don Harrison termed these pairs on any one axis as Mirror Images®. Whichever Abnormal postures were found to exist in the patient, these postures would be placed into their Mirror Image® before a force was applied with an adjusting instrument, drop table, exercise and/or traction.
Figure 8. The possible postural rotations (Rx, Ry, Rz) of the head rib cage and pelvis are depicted in 3-dimensions. In 1980, Dr. Don Harrison termed these pairs on any one axis as Mirror Images®. Whichever postures were found to exist in the patient, these postures would be placed into their Mirror Image® before a force was applied with an adjusting instrument, drop table, exercise and/or traction.
The postural and spinal displacements are the determining factors for deriving a patients individualized program of care. Prior to performing CBP® Mirror Image® postural set-ups, the patients initial presenting abnormal posture(s) must be exactly determined. Ideal posture can be precisely described as vertical alignment of the centers of mass of the head, ribcage, and pelvis with respect to gravity (Figure 1 above). In other words, none of the rotations and translations in Figures 7 and 8 can be present. Using this definition, abnormal postural rotations and translations can be determined.
Mirror Image® Postural Adjustments
In March 1980, Dr. Don Harrison originated postural Chiropractic adjusting procedures that he coined Mirror Image®. Clinically, these adjusting set-ups were found to result in postural and spinal alignment improvements verified with follow up x-ray; this impression would be subjected to studies later as shown in Table 1 above.
For each of these postures illustrated in Figures 7 and 8, Dr. Don Harrison and his brother Glenn Harrison originated drop table adjustments, instrument adjustments (both table and hand-held). For these new Mirror Image® patient positions, Dr. Don Harrison placed the patient in their opposite posture. These Harrison Mirror Image® positions can be described as reflecting the patients head, rib cage, and/or pelvis across the median-sagittal plane in the AP view, and positioning the head, rib cage, and/or pelvis across the mid-frontal plane in the lateral view.9 Figures 9 and 10 demonstrate two examples (there are literally thousands more as there can be many postural combinations of each region) of Mirror Image® Adjustments utilized in CBP® Technique.
Mirror Image Adjustments, assists the Chiropractor in the rehabilitation of the patients posture. In theory, these adjustments re-balance the bodies sense of proper balance or alignment by way of triggering improved muscle and nerve reflexes. Thus, postural adjustments as performed with drop table, hand-held instrument, or even mirror image manipulation procedures, are performed for resetting the nervous system regulation of postural muscle balance.51
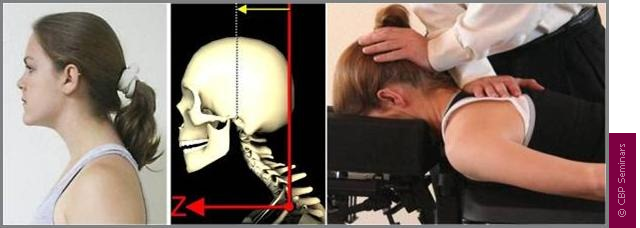
Figure 9. Mirror Image adjustment example for the head posture. The patient has forward head posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is the CBP Mirror Image adjustment. The posture is placed in its opposite position and then a Chiropractic adjustment is performed.

Figure 10. Mirror Image adjustment example for the ribcage posture. The patient has right lateral ribcage posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is the CBP® Mirror Image adjustment. The posture is placed in its opposite position and then a Chiropractic adjustment is performed.
Mirror Image® Postural Exercises
Further, in 1980-1986, Dr. Don and Dr. Glenn Harrison began developing and testing Mirror Image®posture exercises.1-3 Mirror image® exercises are performed to stretch shortened muscles and to strengthen those muscles that have weakened in areas where postural muscles have adapted to asymmetric abnormal postures. Although strength and conditioning exercise has not proven to correct posture,46 postural exercises performed in the mirror image have shown initial promise in the reduction of posture and spinal displacements.47-50 Figures 11 and 12 demonstrate Corrective Mirror Image exercises for the same postures as in Figures 10-11.

Figure 11. Mirror Image exercise example for the abnormal forward head posture. The patient has an abnormal forward head (translation) posture and the skeletal animation shows what happens to the spine with this posture. On the right is two different CBP® Mirror Image exercisesone with just the patients muscles and body as resistance and the other with an elastic band for increased contraction effort. The patient actively maneuvers their posture into the opposite or Mirror Image position.
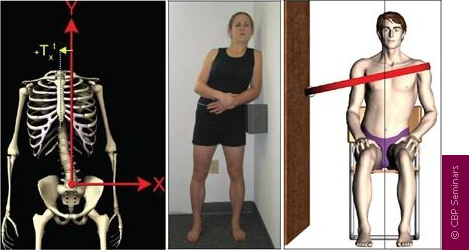
Figure 12. Mirror Image exercise example for an abnormal lateral shifted (translated) ribcage posture. The patient has right lateral ribcage posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is two different CBP® Mirror Image exercises one with just the patient s muscles and body as resistance and the other with an elastic band for increased contraction effort. The patient actively maneuvers their posture into the opposite or Mirror Image position.
Mirror Image® Postural and Spinal Traction
Additionally from 1980-1986, for use in difficult cases, Dr. Don Harrison and Dr. Glenn Harrison originated several Mirror Image® postural traction (rotations and translations of the head, rib cage, and pelvis) and cervical extension (backwards bending) traction methods to restore the sagittal cervical curve. These CBP® Technique cervical extension traction methods were improved upon over the years by several other CBP® practitioners.
From 1996-2000, several postural and spinal traction methods to restore thoracic and lumbar sagittal curvatures were developed by Dr. Deed Harrison; Dr. Don Harrisons son.11-13 Dr. Deed began to further refine the CBP® Technique cervical traction methods with an analysis of head posture, curve configuration, thoracic curvature, gender, and body size.4 From 1992-2004, six non-randomized clinical control trials,13-18 one randomized clinical control trial,19 and five case studies20-24 have been performed on these CBP® Technique Mirror Image® procedures.
Postural mirror image and extension traction for the side view spinal curves provides sustained loading periods of 10-20 minutes and is necessary to cause visco-elastic deformation to the resting length of the spinal ligaments, muscles, and discs.52 In clinical controlled trials, extension traction, as done in CBP® Technique, is the only proven method (without surgery) shown to consistently correct abnormal spinal curvatures back towards their normal alignment.
There are MANY types of spinal extension traction methods used in CBP® Technique; some are more aggressive and technical than others. Whereas some forms of spinal extension traction are available for patients to use at home; the examples shown in Figures 13-14 are in office types only. Note: Each patients spine is unique and thus, a variety of traction devices are used depending upon the exact condition of the patient.
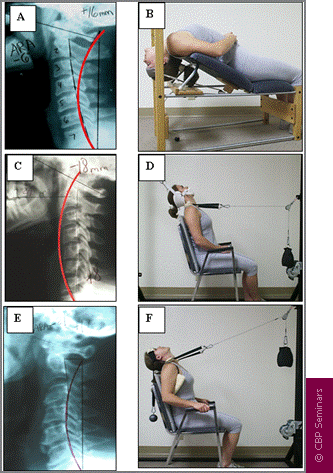
Figure 13. Three different subluxations (abnormal alignment) of the cervical curve and their respective Mirror Image traction methods. In A, hypolordosis with mild anterior head translation requires compression extension traction in B. In C, slight kyphosis with posterior head translation requires 2-way non-compression traction in D. In E, reversal of the upper cervical curve with mild anterior head translation requires compression extension 2-way traction in F.4,14-16
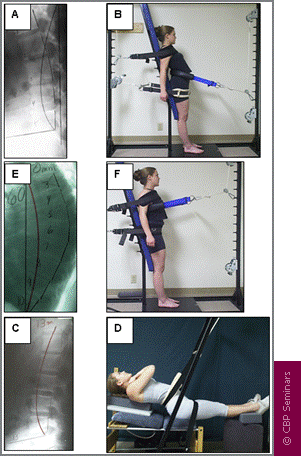
Figure 14. Two different subluxations of the lumbar curve and one of the thoracic curve and their respective Mirror Image traction methods. In A, lumbar kyphosis with anterior thoracic translation requires 3-point bending extension traction in B (shown standing). In C, slight lumbar kyphosis with posterior thoracic translation requires 3-point bending in D (shown supine). In E, hyper-kyphosis of the thoracic curve requires 3-point bending thoracic traction in F (shown standing).
Treatment Interventions
The CBP® protocol of care recommends that relief care (traditional chiropractic management) be separated from structural rehabilitation of the spine and posture. In this regard, the typical patient would receive an initial 3 weeks of care (4 times per week or 12 visits) aimed at improving segmental and overall spinal range of motion (RoM) and pain intensity/frequency. Treatment interventions/methods would consist of any number of segmental adjusting techniques the chiropractor prefers to utilize (Diversified, Gonstead, Activator, etc ).
After, the initial relief care examination (average 12 visits), CBP® structural rehabilitation procedures would begin and include Mirror Image® exercises, adjustments, and traction (referred to as the E.A.T protocol). The mirror image® posture positions are the rotation and translation pairs in or about each coordinate axis (Figures 3 and 4 above). Thus, CBP® care is multi-modal and is consistent with Bolton’s ideas of clinical applications in evidence based practice.45 Table 2 outlines treatment interventions recommended by CBP® for each of relief and structural rehabilitative care.
The reason for postural mirror image exercises, adjustments, and traction procedures is to address all the tissues involved in spine and posture alignment.
Unlike the relief care phase (approximately 12 visits), which includes segmental adjusting procedures from other named techniques, the E.A.T corrective care protocol is unique to CBP®. In combination, these E.A.T. methods are unique to CBP® Technique.
Table 2
CBP® recommended treatment methods for each phase of care, relief and structural rehabilitation of the spine and posture.
Relief Care or Standard Chiropractic Care |
CBP® Technique Structural Rehabilitation
|
||
| Intervention | Determination | Intervention | Determination |
| Spinal Manipulative Therapy | Palpatory Pain and Range of Motion | Mirror Image® Adjustment | PosturePrint® & Clinical Visualization |
| Spinal Stretching | Range of Motion | Mirror Image® Exercise | PosturePrint® & Clinical Visualization |
| Ice / Heat | Injury / Inflammation | Mirror Image® Postural Traction | PosturePrint® & Clinical Visualization |
| Mirror Image® Sagittal Curve Traction | Lateral View X-Ray (PostureRay® X-Ray Digitalization Preferred) | ||
Frequency & Duration of CBP® Technique Care
Previously it was stated that a typical patient is started with relief care at a frequency of 4 times per week for 3 weeks or 12 visits. After this 12 visit relief care regiment, a patient is re-evaluated to document improvements in initial (visit 1) positive exam findings, pain scales, disability indices, health status, and range of motion. Following this re-evaluation, the patient is transitioned into CBP® structural rehabilitative E.A.T. procedures.4
To determine if the CBP® E.A.T protocol of corrective care for each individual (based on his/her posture and spinal displacements) is achieving the desired normalization of posture and spinal alignment, re-examinations are suggested at 36 visit intervals. In other words after 24 visits of CBP® E.A.T interventions added to the initial 12 visits of relief care. This 36 visit number is not based on personal opinion, but rather is an average duration from our six CBP® clinical control trials.13-18 In order to arrive at this 36 visit time period, one could use a frequency of 4 visits per week for 9 weeks or 3 visits per week for 12 weeks.
In six clinical control trials detailing the outcomes of chronic pain patients with CBP® Treatment interventions, the average chronic pain patient achieved a 75-80% improvement in their chronic pain and a 50% correction of their initial subluxated (abnormal spine alignment) position towards ideal and average spine alignment.13-18 This data indicates that, on average, a typical chronic pain patient may need 2 blocks of 36 visits of intensive structural rehabilitative care (defined as 3 or 4 visits per week) to achieve as near normal spinal alignment as possible.
Table 3
CBP® Protocol and Phases of Care showing the timing of different Treatment methods.
The frequency and duration of further care recommended to the patient at the 36 visit re-evaluation depends on their improvement in both structural and functional based outcomes. For example, if a patient achieves near-normal posture and spinal alignment at the 36 visit re-evaluation, then a reduced frequency of treatment is recommended for stabilization care (1-4 times per month depending upon the case). However, if at the first corrective care re-evaluation, less than average improvement is attained on comparative radiographs and postural examination (PosturePrint), then this is indication that another block of 36 visits may be necessary for continued spinal correction. With CBP®’s six completed clinical control trials, our methods have moved from the clinical opinion arena to having foundation in the category of evidence based care.
Conclusion
In our present era, evidence-based medicine was coined as a means to improve patient outcomes and quality of care. CBP® Technique uses postural and radiographic analysis procedures that have been shown to be reliable and valid. Significantly, CBP® Technique has multiple types of peer-reviewed publications in scientific journals as evidence for its patient treatment methods. What remains for CBP® technique is further refinement of technique protocols and evaluating the effects of subluxation reduction using the E.A.T. procedures in more advanced study designs. CBP is a technique practiced by a large number of practitioners, is a leader in the chiropractic technique and biomechanics research arena, and has shown good potential to improve chronic pain conditions in several patient populations and selected case studies.


CONTACT CBP
CBP Seminars, Inc.
21863 Thorsten Avenue Suite 207
Caldwell, ID 83605
Phone: 208-939-0301
Fax: 208-209-6009
Email: [email protected]
Web: idealspine.com
LATEST ARTICLES
CONTACT CBP
CBP Seminars, Inc.
1160 Taylor Street Suite 100
Meridian, ID 83642
Phone: 208-939-0301
Fax: 208-209-6009
Email: [email protected]
Web: idealspine.com